Loading...
albaniahairclinicFOLLOW US


#1 In Albania
Albania Hair Health Center is a globally renowned hair transplant brand based in Albania, renowned for delivering high-quality FUE, DHI, and Sapphire FUE procedures at competitive and affordable prices, with international offices providing personalized support, multilingual teams, and comprehensive packages for clients worldwide seeking natural, permanent results.








One of the primary reasons patients from all over the world choose Albania for their hair transplant procedures is the cost. Hair transplant in Albania offers significant savings compared to other countries, without compromising on quality. At Albania Hair Clinic, we provide transparent pricing with no hidden costs, ensuring you get the best value for your money.
Albania Hair Medical Center stands out for its commitment to excellence and patient satisfaction. We use the latest technologies and techniques to ensure natural-looking results. Our team of experienced surgeons and medical staff are dedicated to providing the highest quality care.



Hair transplant procedures in Albania are significantly more affordable compared to many developed countries, making the country an increasingly popular destination for patients seeking high-quality hair restoration. Albania has built a strong reputation for delivering internationally recognized standards of care at costs that are often several times lower than those found in Western Europe, the UK, or the United States.
The overall price of a hair transplant in Albania depends on multiple factors related to the individual treatment plan. One of the primary elements influencing cost is the total number of grafts required to adequately cover the thinning or bald areas. Pricing may also vary depending on the clinic’s reputation, the surgeon’s level of experience, the techniques used, and the scope of services included within the treatment package.
Albania has become a preferred hub for hair transplant procedures, offering advanced solutions for hair loss supported by experienced medical teams and modern clinical environments.
The combination of competitive pricing, qualified specialists, and contemporary medical facilities has positioned Albania as a leading destination for hair transplant treatments, attracting patients from across Europe and beyond who are seeking reliable, effective, and affordable hair restoration options.
We provide a comprehensive selection of hair restoration solutions, including FUE hair transplants to redefine and strengthen your hairline, beard transplants to create thicker and more even facial hair, and eyebrow transplants to achieve a fuller, well-shaped appearance.
If you are experiencing hair thinning or baldness, you are certainly not alone. Androgenetic alopecia, widely known as male pattern hair loss, affects nearly 30% of men by the age of 30 and approximately 50% by the age of 50. Our goal is to support you in regaining both your confidence and a stronger, more natural-looking hairline.
Hair restoration is not limited to men. We also offer specialized female hair transplant procedures, targeted hair loss treatments, and eyebrow restoration options designed to rebuild sparse or over-plucked brows, helping patients achieve balanced and natural results.

3 months ago
It's very hard for me to describe every single person of the group because all of them were so kind and so respectful especially there work is just amazing I'm so happy that I did my hair transplant with Albania hair clinic thanks to all the team

4 months ago
Very good experience. Very professional team. The hotel is located in the same complex as the clinic. I recommend it.

4 months ago
The experience and the staff treatment was grateful. Really recommended. Coming back here to share the results

5 months ago
Very good experience. They are very professional and attentive. All promises were clearly maintained. During my hair transplant, the nurses were focused and caring throughout the procedure. The accommodation they arranged was comfortable and well organized. While performing the transplant, they listened carefully to my concerns about specific areas and worked according to my expectations. They delivered the number of grafts they promised and the process was handled transparently. I highly recommend them.

12 months ago
From start to finish, my experience was amazing. The doctor explained everything in detail, and the recovery was quicker than I expected. Seeing my hair grow back has been life-changing!"
0.0
Average Rating
Over
0
Total Reviews
Over
0
Years of Experience
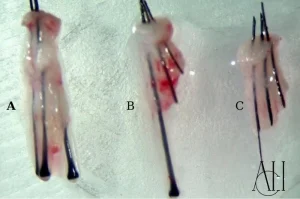
Witness stunning before and after hair transplant results from our Tirana Medical Center, showcasing advanced methods like FUE, DHI, and Sapphire FUE that deliver natural density and scar-free recovery for patients traveling from Rome, Italy, and beyond Europe. See how Italian clients achieve fuller hairlines and renewed confidence, inspiring your decision to choose our expert care for transformative, personalized results.

When it comes to hair transplant cost in Albania, especially in Tirana, few clinic offer the perfect balance of affordability, advanced medical standards, and personalized patient care like Albania Hair Clinic. While countries such as the USA ($8,000–$30,000), the UK ($4,500–$10,000), and Western Europe come with significantly higher price tags, Albania stands out as one of the most cost-effective destinations in Europe. At Albania Hair Clinic in Tirana, we provide premium hair transplant procedures including advanced FUE, DHI, and Sapphire FUE techniques — delivering natural, long-lasting results at highly competitive prices. Our expert medical team, modern facilities, and patient-focused approach ensure world-class quality without the financial burden seen in other countries.
For those seeking the most successful and natural-looking results, Albania Hair Clinic stands as your number one choice. With over 12 years of expertise, our globally recognized team delivers exceptional hair transplant outcomes that combine advanced medical technology with an artistic touch. Every procedure is customized to your unique features — ensuring a seamless, natural appearance that enhances your confidence and reflects who you truly are. From consultation to recovery, we provide a personalized, world-class experience that thousands of patients from around the world trust and recommend.


Speak with our expert DHI Hair Transplant specialist We're ready to answer your questions





Page 1 of 10